IGMIN: We're glad you're here. Please click 'create a new query' if you are a new visitor to our website and need further information from us.
If you are already a member of our network and need to keep track of any developments regarding a question you have already submitted, click 'take me to my Query.'
Welcome to IgMin Research – an Open Access journal uniting Biology, Medicine, and Engineering. We’re dedicated to advancing global knowledge and fostering collaboration across scientific fields.
At IgMin Research, we bridge the frontiers of Biology, Medicine, and Engineering to foster interdisciplinary innovation. Our expanded scope now embraces a wide spectrum of scientific disciplines, empowering global researchers to explore, contribute, and collaborate through open access.
Welcome to IgMin, a leading platform dedicated to enhancing knowledge dissemination and professional growth across multiple fields of science, technology, and the humanities. We believe in the power of open access, collaboration, and innovation. Our goal is to provide individuals and organizations with the tools they need to succeed in the global knowledge economy.
IgMin Publications Inc., Suite 102, West Hartford, CT - 06110, USA
Objective: We compared the prevalence of abnormal glucose status between Senegalese migrants and their relatives staying in their villages in Fuuta (a rural region in the Northern part of Senegal).
Design and methods: We led an exhaustive study on all the Senegalese migrants present in Saint-Die (Vosges, France) (SD) at a 1-year interval. We led a similar study at the same period on their relatives in their villages of Fuuta (F). Study parameters were Weight (W), height, Body Mass Index (BMI), Waist/Hip Ratio (WHR), and Fasting Capillary Glycaemia (FCG) expressed in total blood glucose. We classified patients into normal (N: FCG ≤ 1.00 g/l), Impaired Fasting Glycaemia (IFG: FCG between 1.00 g/l and 1.09 g/l), diabetic (D: FCG > 1.10 g/l when fasting or ≥ 1.80 g/l when not fasting), or abnormal glucose status (IFG + D). SD sample included 74 subjects (58.1% female) of mean age 41.7+/-12.7 years. The sample included 847 subjects (66.9% female) of mean age 37.3+/-17.8 years.
Results: In the SD group, W was 76.8+/-11.4 kg (BMI = 26.80+/-4.30 kg/m2); 57 (77.03%) had normal blood glucose, and 17 (22.97%) had IFG+D, among whom 12 (70.6%) were diabetic. In the F group, W was 60.8+/-10.9 kg (BMI = 21.37+/-3.70 kg/m2); 791 (93.39%) had normal blood glucose, and only 56 (6.61%) had IFG+D, among whom 35 (62.5%) were diabetic. Prevalence of IFG+D between SD and F was significantly different (p < 0.01%). There are still significant differences after standardization on age.
Conclusion: As described in other countries, Senegalese migrants have a much higher risk of developing diabetes mellitus than their relatives remaining in their birth country. The main reason seems to be the nutritional transition (diet and sedentary lifestyle).
Type-2 Diabetes (TD-2) is an increasing problem in sub-Saharan Africa [11Mbanya JCN, Sobngwi E, Assah FK, Enoru ST. Diabetes in sub-Saharan Africa. Lancet. 2010;375:2254-66. PMID: 20609971]: prevalence and burden are rising very quickly as a consequence of major lifestyle changes. In 2009, the International Diabetes Federation [22Diabetes atlas (4th edn). International Diabetes Federation, 2006.] projected a 98% growth in the number of diabetic adults in this region and a 54% increase in the world. Beyond the ketosis-prone atypical diabetes [33Sobngwi E, Mauvais-Jarvis F, Vexiau P, Mbanya JCN, Gautier JF. Diabetes in Africans, part 2: ketosis-prone atypical diabetes mellitus. Diabetes Metab. 2002;28:5-12.], the main cause of diabetes in Africa, as everywhere, is Impaired Glucose Tolerance (IGT) in relation to epidemic obesity [44Sarr A, Lopez-Sall P, Ndour-Mbaye NM, Diop SN, Sarr GN, Diop O, et al. Frequency of metabolic syndrome in Black Africans, in Senegal. Médecine des Maladies Métaboliques. 2012;6-3:238-43.-66Fontbonne A, Favier F, Papoz L. Type 2 diabetes in the world: analysis of an epidemic. Journ Annu Diabetol Hotel Dieu. 2003. PMID: 12868301]. The main causes are urbanisation and economic and nutritional transition [77Osei K, Schuster DP, Amoah AGB, Owusu SK. Diabetes in Africa. Pathogenesis of type 1 and type 2 diabetes in sub-Saharan Africa: implications of transitional populations. J Cardovasc Risk 2003;10:85-96. PMID: 12668905]. In Senegal (West Africa), it has already become a great problem in the main city, Dakar, and its suburbs, even though there are still some doubts about the differences between men's and women's diabetes risks [88Fontbonne A, Cournil A, Cames C, Mercier S, N’Diaye-Coly A, Lacroux A, et al. Anthropometric characteristics and cardiometabolic risk factors in a sample of urban-dwelling adults in Senegal. Diabetes Metab. 2011;37:52-58. PMID: 21112227]. In the villages, the way of life is very different (physical labour, agricultural work, little electrification…) and diabetes is still unknown. In our hospital, we have remarked that the Senegalese migrants (in the majority coming from Fuuta, the Northern region along the Senegal River) have a very high prevalence of IGT or TD-2 (unpublished data). Similar trends have been reported among several migrant populations in Europe [99Osei K, Schuster DE. Metabolic characteristics of African descendants: a comparative study of African-Americans and Ghanaians immigrants using minimal analysis. Diabetologia. 1995;38:1103-1109. PMID: 8591826-1414Fujimoto WY. The growing prevalence of non-insulin-dependent diabetes in migrant Asian populations and its implications for Asia. Diabetes Res Clin Pract. 1992;15:167-183. PMID: 1563334] as well as around the world [1515Delcourt C, Papoz L. Diabetes and its complications in the French population. Editions Inserm. 1996.-1717Henson JJ, Gray LJ, Khunti K, Guru A, Misra A, Davies MJ. The impact of migration on metabolic outcomes and coronary heart disease risk: a comparison of migrant South Asians, Asian Indians and white Europeans. Diabetologia 2010;53:S354.].
This study aimed to compare the prevalence of abnormal glucose status between the Senegalese migrants in France, especially around Saint-Dié (Vosges, France), and their relatives dwelling in their village in Fuuta. Our objective is to find out whether the migration can lead to an increase in prevalence among Senegalese migrants.
We studied adult people of both sexes, older than 18 years, who had agreed to be tested. Pregnant women were not included.
The present study involved 2 different populations. Firstly, an exhaustive study was conducted among the Senegalese migrants in Saint-Dié (SD group). To be sure to be exhaustive, we took the help of census data. We have conducted this study in two phases at a 1-year interval. People were tested at home between 07 and 09 AM, in a fasting state, before breakfast. This SD-group included 87 subjects, but we have only kept 74 subjects who were surely in a fasting status. Secondly, we studied the adult population of 5 villages in Fuuta (F group), the region of Senegal from which the Saint-Dié migrants came. It is a rural country, very far from capital Dakar (more than 800 km), without hospitals or medical laboratories. These 5 villages were: Bapalel, Gouriki, Hordolde, Soringho, and Thially. Villages had been informed of our study three months before and of our precise coming the day before by the chief of the village and/or the community health worker. We didn’t have the use of precise civil status data in these villages. So, according to the way of life in these villages, we have chosen the cluster sampling method: in each village we have drawn lots 3 streets and our team was divided into 3 groups (one group for one street: one medical doctor, one nurse and one interpreter) that followed these 3 streets from the centre of the village to the end; along these streets, we studied all the adults corresponding to the selection criteria in every compound. The F-group included 1263 subjects (189 from Bapalel, 222 from Gouriki, 311 from Hordolde, 310 from Soringho, and 241 from Thially). For the analysis, we have secondarily eliminated the subjects whose fasting status was doubtful, except if they were surely diabetic; so, we have only kept 847 subjects.
Parameters
All the tests were done in the morning, between 07 and 13 AM, in November and December 2000 (SD and F) and 2001 (SD). Selected subjects told us to be fasting for more than 12 hours without our opportunity to check it.
For all the selected adults, we recorded their sex and age. We measured four anthropometric parameters: height (cm), weight (kg), Body Mass Index (BMI, kg/m2), and Waist/Hip Ratio (WHR).
As it was not possible to perform venous glycaemia or glucose tolerance tests in the villages (lack of laboratories), we opted for only capillary glycaemia both for SD and F. We measured the Fasting Capillary Glycaemia (FCG) using a Glucotrend lector (Lab. Boehringer) after a pick with Softclix autopicker. The subjects with abnormal glycaemia were every time re-interrogated about their fasting status and re-tested the day after to ensure that this was really abnormal. In these cases, we only took into account the second FCG.
Glucotrend lector gave results in “total blood glucose”. The criteria of normal or abnormal glycaemia are nowadays explained in “plasma glucose”, no more in “total blood glucose” (11% lower than plasma glucose). According to this transformation and to the international criteria of WHO and ADA (gave in plasma glucose in 2006), did not use blood glycaemia for the comparisons but the belonging to one of the 3 commonly recognised classes to define glucose status: Normal (N) with FCG ≤ 1.00 g/l; Impaired Fasting Glycaemia (IFG) with FCG between 1.00 and 1.09 g/l; and Diabetic (D) with FCG ≥ 1.10 g/l. When there was a doubt about fasting status (casual), we considered as diabetic a subject with FCG > 1.80 g/l..
Statistical methods
Q, quantitative data are given as mean+/-sd.
Comparisons between anthropometric parameters were analysed by Student's t-test. Percentages were compared by chi2-test with Yates correction applied if relevant.
Correlations between age, BMI, and waist/hip ratio were analysed by the Fisher method with an α risk of 5%.
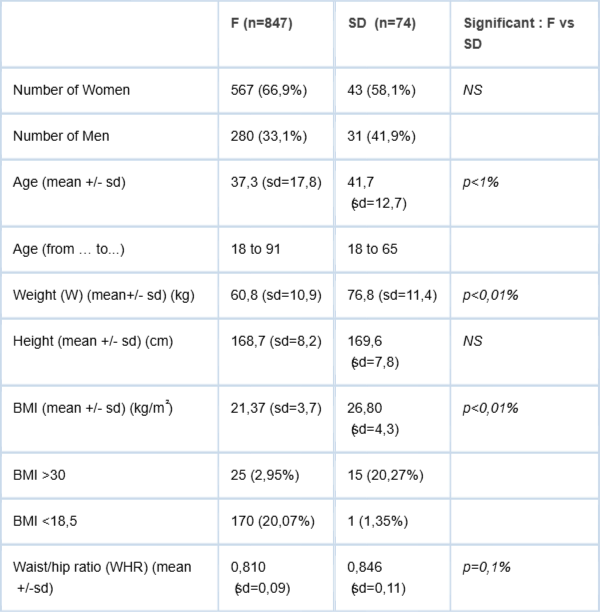
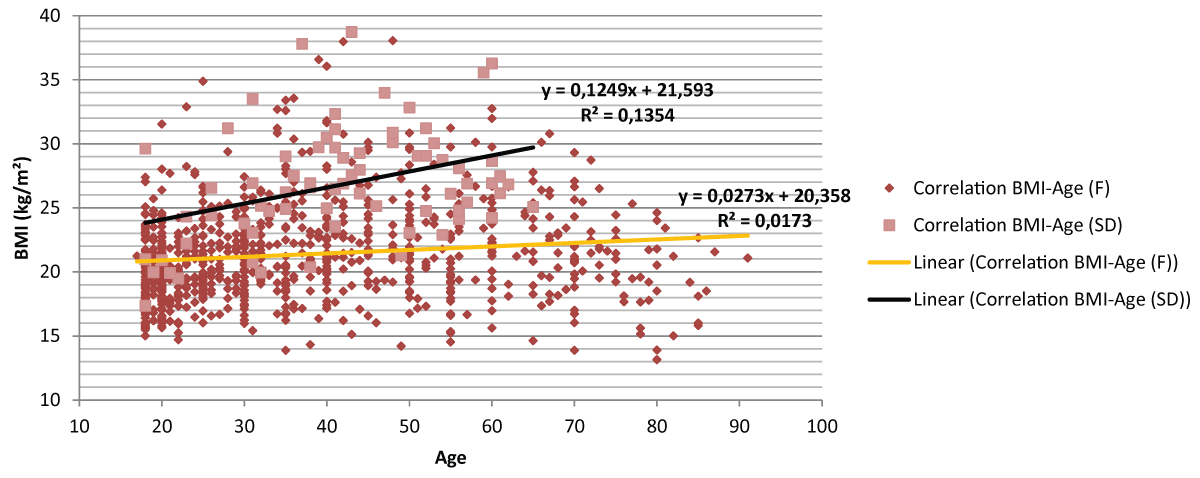
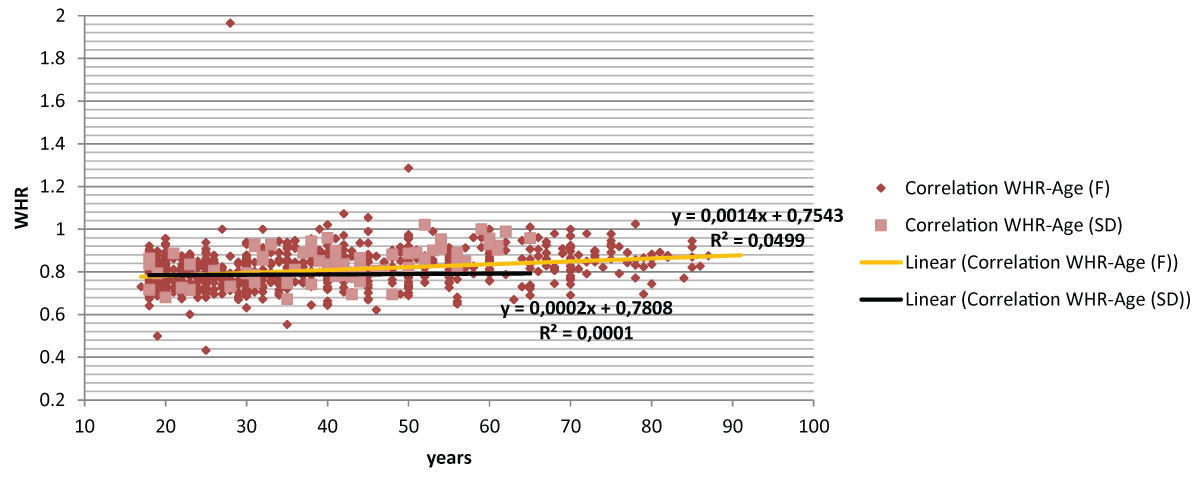
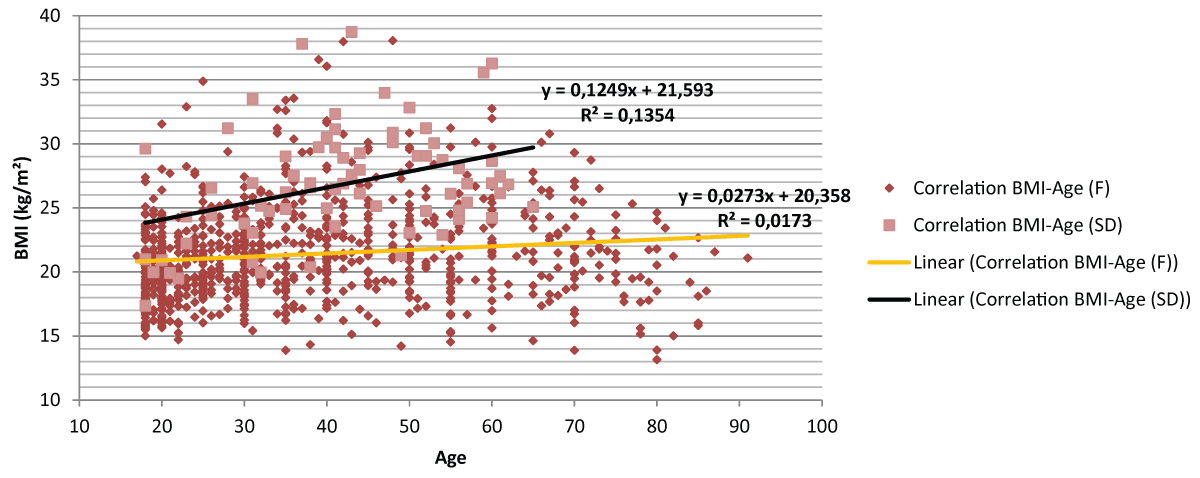
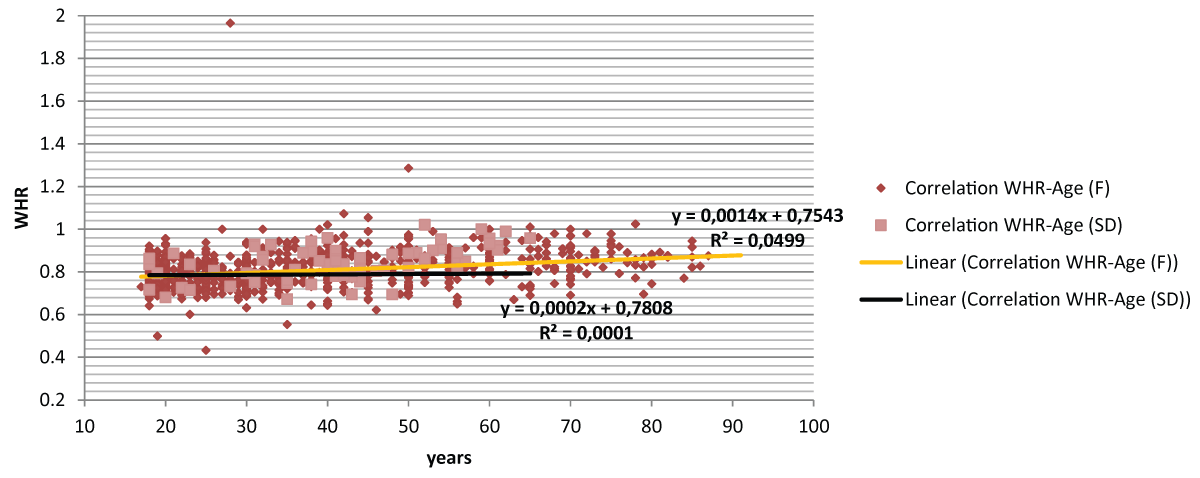
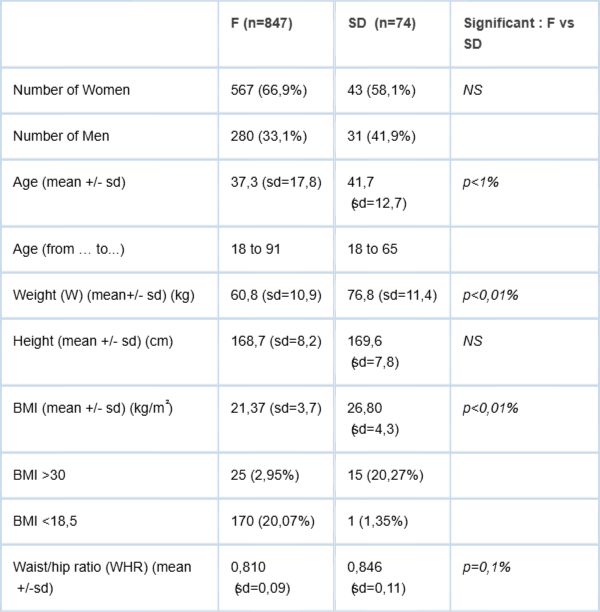
The characteristics of the 2 populations are described in Table 1. SD and F were not statistically different for height (169.6+/-7.8 cm versus 168.7+/-8.2 cm, respectively) and for sex-ratio (female: 58.1% versus 66.9%, respectively). SD-group was significantly older (41.7+/-12.7 years versus 37.3+/-17.8 years), heavier (76.8+/-11.4 kg versus 60.8+/-10.9 kg), and with a greater BMI (26.80+/-4.30 kg/m2versus 21.37+/-3.70 kg/m2). There was significantly more android obesity in the SD-group than in the F-group. As shown in Figure 1, there were significant correlations between age and BMI in the two groups, but the correlation was stronger (p < 0.1%) in the SD group (r2 = 0.135) than in the F group (r2 = 0.017). The same results were observed for WHR and age (Figure 2, p < 0.01).
Table 1: Baseline characteristics of the 2 studied populations ( F for Fuuta / SD for Saint-Die).
Figure 1: Correlation between BMI and age (years) in Fuuta (F) and Saint-Die (SD).
Figure 2: Correlation between WHR and age (years) in Fuuta (F) and Saint-Die (SD).
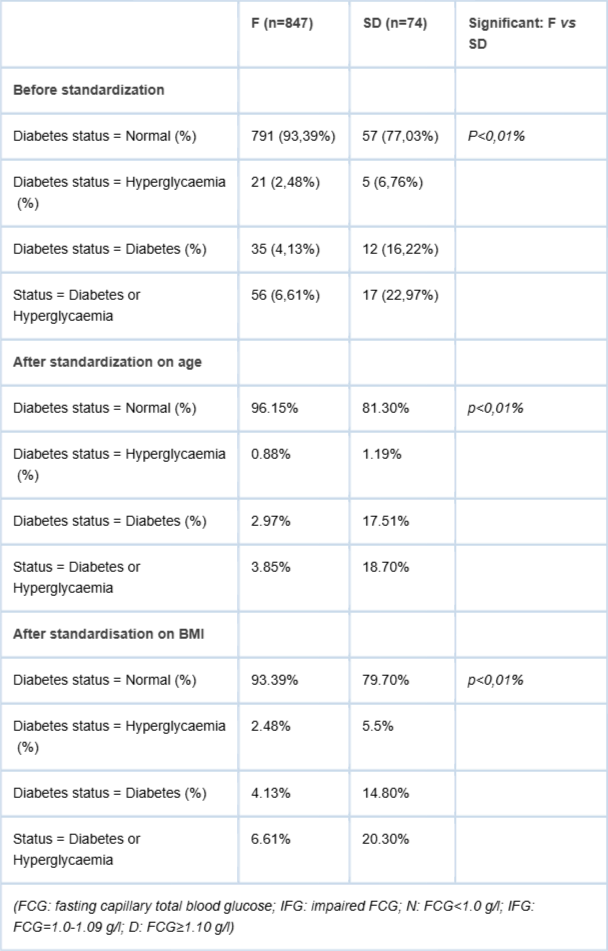
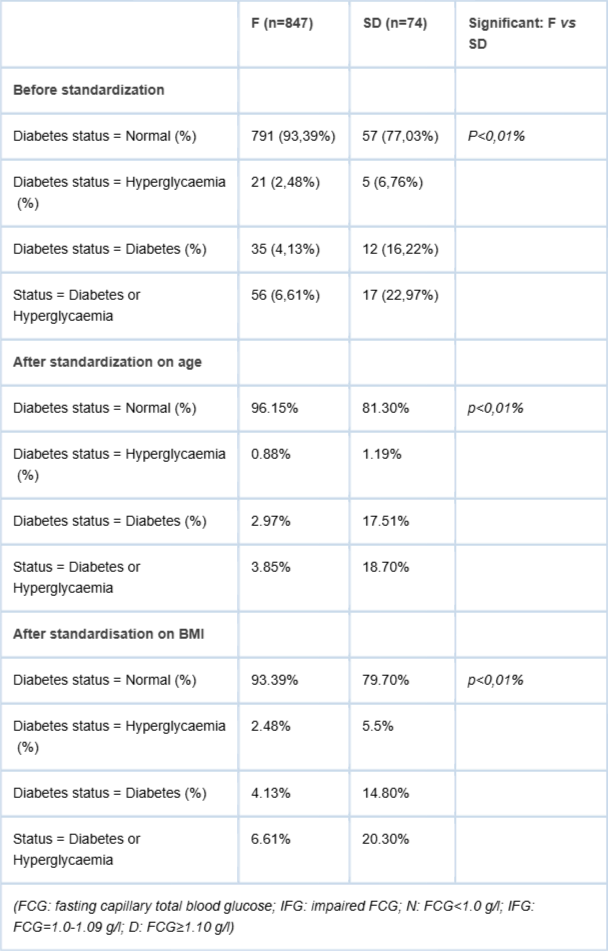
Table 2 shows the results of the glucose status of our 2 populations. Out of the 74 subjects tested in the SD-group, 57 (77.03%) were normal, 5 (6.76%) had IFG (3 females and 2 males), and 12 (16.22%) had diabetes (4 females and 8 males). In the F-group, out of the 847 subjects, 791 (93.39%) were normal (527 females and 264 males), 21 (2.48%) had IFG (15 females and 6 males), and 35 (4.93%) had diabetes (18 females and 17 males). There were more pathological subjects (IFG+D) in SD than in F (22.97% versus 6.61%). The standardization of age and BMI didn’t modify these differences, which remain significant. When considering 3 classes of age (18-39 years, 40-59 years and above 60 years), at each age class there were statically more pathological (IFG+D) subjects in SD group than in F group (in 18-39 years class: 19.35% in SD and 4.00% in F; in 40-59 years class: 20.0% in SD and 11.05 in F; in more 60 years class: 50.0% in SD and 10.68% in F). Great %ages (> 10%) appear sooner in SD (since 18-39 years) than in F (after 40 years).
Table 2: Results on glucose status for the 2 studied populations (F for Fuuta / SD for Saint-Die).
This study is the first French study comparing the frequency of glucose abnormalities between a population of migrants and the population remaining in their birth villages. It was carried out in Senegal and in France with the same light way (capillary and not venous glycaemia and no glucose tolerance test). This method, particularly capillary glycaemia, has already been used in similar studies, in particular in Mauritania [1818Ducorps M, Baleynaud S, Mayaudon H, Castagne C, Bauduceau B. A prevalence survey of diabetes in Mauritania. Diabetes Care. 1996;19:761-763. PMID: 8799635], a neighbouring country of Fuuta.
To interpret our results, it is necessary to take into account the potential bias of recruitment. For SD, the population was studied in an exhaustive way, and the sex ratio shows a number of women (58.1%) less than that of the F population (66.9%). In Fuuta, it was necessary to sample the population according to a method recognized in Public Health (method of the bunches): the proportion of women in the F-group is higher than in the SD-group, probably because many men of the villages had migrated to Europe, and many of the others were in their fields at the time of our passage. Nevertheless, this difference is not significant. However, the main skew liable to affect our study was the incomplete knowledge of the fasting status of the subjects at home. This is the reason why we have eliminated 416 subjects (32.9%) in the F-group and only 14 (16.1%) in the SD-group whose fasting status was not sure.
The definitions of obesity or simple overweight are also problematic in a black population. While for the Caucasian subject the limits are clear [1919Basdevant A, Laville M, Ziegler O. Practice guideline for the diagnosis, prevention, treatment of obesity in France. Diabetes Metab. 1998;24:10-42. PMID: 9805639], there is still a debate on the best limits to apply for the black subjects [1111Okosun IS, Cooper RS, Rotimi CN, Osotimehin B, Forrester T. Association of waist circumference with risk of hypertension and type-2 diabetes in Nigerians, Jamaicans, and African-Americans. Diabetes Care. 1998;11:1836-1842. PMID: 9802730,2020Summer AE, Kushner H, Tulenko TN, Falkner B, Marsch JB. The relationship in African-Americans of sex differences in insulin-mediated suppression of nonesterified fatty acids to sex differences in fasting triglyceride levels. Metabolism. 1997;46:400-405. PMID: 9109843]: to avoid this pitfall, we took into account the absolute values of BMI and waist/hip ratio, and not only a stratification of BMI into 3 classes. The study by Okosum [1111Okosun IS, Cooper RS, Rotimi CN, Osotimehin B, Forrester T. Association of waist circumference with risk of hypertension and type-2 diabetes in Nigerians, Jamaicans, and African-Americans. Diabetes Care. 1998;11:1836-1842. PMID: 9802730] shows that the waist measurement is a better marker of the risk of diabetes for the Nigerian immigrants in the USA than for the Nigerians remained in their villages. We found the same trends in our population where the correlation between BMI (or the waist/hip ratio) and age is stronger for SD than F (Figure 1 and 2). Irrespective of the mode of definition of obesity, there are significantly more android obese subjects in SD than in F. The percentage of obese people in SD (20.3%) is much higher than %age of metabolic syndrome in Dakar (8.9% -in 4).
The prevalence of the glycoregulatory disorders is of 6.61% in the villages of our study (F). It is higher than the mean data (less than 3.0%) in Mbanya’s review [11Mbanya JCN, Sobngwi E, Assah FK, Enoru ST. Diabetes in sub-Saharan Africa. Lancet. 2010;375:2254-66. PMID: 20609971]. It is interesting to note in this review that the more recent the study, the higher the prevalence of diabetes because of the dramatic increase in the epidemic even in Africa. The results of our study in 2000 conform with those of recent studies in Africa: Tanzania [2121McLarty DG, Unwin N, Kitange HM, Alberti K. Diabetes mellitus as a cause of death in sub-Saharan Africa: results of a community-based study in Tanzania. The Adult Morbidity and Mortality Project. Diab Med. 1996;13:990-994. PMID: 8946159] or Ghana [2222Motala Ayesha A, Omar Mohammed AK, Pirie FJ. Diabetes in Africa. Epidemiology of type 1 and type 2 diabetes in Africa. J Cardiovasc Risk. 2003;10:77-83. PMID: 12668904]. In each recent study, it was found the same level of prevalence of diabetes (3-6%) was found in the rural populations. A study carried out 15 years before in Mauritania [1818Ducorps M, Baleynaud S, Mayaudon H, Castagne C, Bauduceau B. A prevalence survey of diabetes in Mauritania. Diabetes Care. 1996;19:761-763. PMID: 8799635] in an ethno-group identical to that of Fuuta, yielded identical results: a diabetes prevalence of 1.8% in a population with an average BMI of 22.7 kg/m2 and 34.6 years as the mean age. We can conclude that the average rate of diabetes in these village-dwelling ethno-groups increases, as everywhere in the world.
Our study shows a significantly higher rate of the glycoregulatory disorders among migrants (SD) than in the village-dwellings (F), even after standardization on age (24.25% at SD versus 6.61% at F) or on BMI (15.05% at SD versus 6.61% at F). There were no significant differences according to sex. Other studies on migrants in developed countries lead to the same conclusion: as in our study, the risk of diabetes increases in a very significant way in parallel with the increase in BMI. For instance, in Cameroon [1616Mbanya JC, Cruickshank JF, Forrester T, Balkau B, Ngogang NY, Riste L, et al. Standardized comparison of glucose tolerance in West-African origin populations of rural and urban Cameroon, Jamaica, and Caribbean migrants to Britain. Diabetes Care. 1999;22:434-440. PMID: 10097925], in 1999, the rate of diabetes in rural environments was lower than 1%, whereas in their immigrant relatives living in Manchester, it was of 14%. These results are similar to those of the African-American minorities in the USA [2323Brancati FL, Kao WHL, Folsom AR, Watson AR. Incident type 2 diabetes mellitus in African American and white adults: the Atherosclerosis Risk in Communities Study. JAMA. 2000;283:2253-2259. PMID: 10807384], where the rate of glucoregulatory disorders (after standardization on age and sex) is of 18.8% compared with 14.4% in the white population living in the same environment. All these results tend to confirm the importance of the way of life (rural versus urban) for the transition from normal status to diabetes. This appears after a little modification of weight. This suggests that black populations have a strong susceptibility to diabetes.
However, the same phenomenon of increasing risk of abnormal glucose tolerance is found in most immigrant populations coming from poorer countries [11Mbanya JCN, Sobngwi E, Assah FK, Enoru ST. Diabetes in sub-Saharan Africa. Lancet. 2010;375:2254-66. PMID: 20609971,24-2724-27Taylor R, Bennet P, Uili R, Joffres M, Germain R, Levy S, et al. Diabetes in Wallis Polynesian: a comparison of residents of Wallis Islands and first-generation migrants in Noumea, New Caledonia. Diab Res Clin Pract. 1985;1:169-178. PMID: 3836104]. The interest of our study is to compare 2 populations coming from the same small area. So, the shown differences can be mainly explained by the effects of migration. It indicates that the migratory phenomenon generates important metabolic disturbances.
There are several possible explanations for this phenomenon. In our study, the differences in lifestyle are obvious between F and SD. Even though we have no quantitative data about the diet of the two groups, we can report observational data. In the villages, the food is monotonous, containing a lot of rice with meat or fish, but few fruits and sweet drinks. These diets are well adapted to the lifestyle in the villages where people engage in substantial physical activity and manual labour in very hot weather. The migrants living in France live downtown, walk little, and are often unemployed or work in a much less physical way. Over more: if the migrants eat traditionally for a few years, quickly, under the pressure of their children and their neighbours, they switch, more and more, to an occidental diet. As they often belong to the disadvantaged classes in their host country, they consume far too much fried food, sweet drinks, and fewer fruits or vegetables [2828Connoly V, Unwin N, Sherriff P, Bilous R, Kelly W. Diabetes prevalence and socioeconomic status: a population-based study showing increased prevalence of type 2 diabetes mellitus in deprived areas. J Epid Comm Health. 2000;54:173-177. PMID: 10746110]. For all these reasons, it is understood that they tend to grow fatter than their relatives in Fuuta at the same age. The same problem has been shown in an urban population in Dakar [44Sarr A, Lopez-Sall P, Ndour-Mbaye NM, Diop SN, Sarr GN, Diop O, et al. Frequency of metabolic syndrome in Black Africans, in Senegal. Médecine des Maladies Métaboliques. 2012;6-3:238-43.].
The duration of immigration is undoubtedly an important factor. Our population of immigrants is composed partly of first-generation immigrants (in France for 30 years), partly of the second generation. If we compare our results with those of the Cameroonian immigrants in Great Britain [33Sobngwi E, Mauvais-Jarvis F, Vexiau P, Mbanya JCN, Gautier JF. Diabetes in Africans, part 2: ketosis-prone atypical diabetes mellitus. Diabetes Metab. 2002;28:5-12., 16 16Mbanya JC, Cruickshank JF, Forrester T, Balkau B, Ngogang NY, Riste L, et al. Standardized comparison of glucose tolerance in West-African origin populations of rural and urban Cameroon, Jamaica, and Caribbean migrants to Britain. Diabetes Care. 1999;22:434-440. PMID: 10097925], there is not a great difference between 22.9% of the glucoregulatory disorders at SD and 30% at the Cameroonian immigrants. It could be explained by the same duration of immigration. It is the same situation for the Ghanaians in the USA [99Osei K, Schuster DE. Metabolic characteristics of African descendants: a comparative study of African-Americans and Ghanaians immigrants using minimal analysis. Diabetologia. 1995;38:1103-1109. PMID: 8591826]. The effect of the “westernisation” of lifestyle [11Mbanya JCN, Sobngwi E, Assah FK, Enoru ST. Diabetes in sub-Saharan Africa. Lancet. 2010;375:2254-66. PMID: 20609971] or “Coke-colonization” [2929Gautier JF, Sobngwi E, Vexiau P. How I treat and manage diabetes in black people. 19e Journées de Diabétologie de l’Hôtel-Dieu. 2001.] takes a long time before being completely expressed: it needs at least two generations for the migrants to give up their traditional practices of life.
Some studies have advanced genetic predispositions of certain black ethnic groups about diabetes [1111Okosun IS, Cooper RS, Rotimi CN, Osotimehin B, Forrester T. Association of waist circumference with risk of hypertension and type-2 diabetes in Nigerians, Jamaicans, and African-Americans. Diabetes Care. 1998;11:1836-1842. PMID: 9802730,30-3130-31Buthelezi EP, Van Der Merwe MT, Lönnroth PN, Gray PI, Crowther NJ. Ethnic differences in the responsiveness of adipocyte lipolytic activity to insulin. Obes Res. 2000;8:171-178. PMID: 10757203]. This would be a question of “over-adaptation”? In France, the exposure of the Fuuta population to facilitating environmental factors results in a very fast emergence of a high rate of glucoregulatory disorders, superior to that of the French population living in the same country (22.97% for SD compared with 3.01% in the population of origin in Vosges-France [3232Ricordeau P, Weill A, Vallier N, Fender P, Allemand H. Epidemiology of diabetes in metropolitan France. Diab Metab. 2001;26:11-24. PMID: 11011236] at the same period). Nevertheless, if there is no obligatory genetic predisposition of this ethno-group to diabetes, these people perhaps have a predisposition to an exaggerated response to the environmental factors for reasons of survival [3333Swinburn BA. The thrifty genotype hypothesis: how does it look after 30 years? Diab Med. 1996;13:695-699. PMID: 8862942]. However, according to Summer [2020Summer AE, Kushner H, Tulenko TN, Falkner B, Marsch JB. The relationship in African-Americans of sex differences in insulin-mediated suppression of nonesterified fatty acids to sex differences in fasting triglyceride levels. Metabolism. 1997;46:400-405. PMID: 9109843], with equal BMI, the African women have less abdominal adipose tissue than the Caucasian women: this could explain why, in a basal state, they would have less risk of developing diabetes.
The environmental differences leading to diabetes in our population of immigrants can be gathered under the term “nutritional transition”. Like the “epidemiologic transition” [55Motala AA. Diabetes trends in Africa. Diabetes Metab Res Rev. 2002;18:S14-S20. PMID: 12324980, 7 7Osei K, Schuster DP, Amoah AGB, Owusu SK. Diabetes in Africa. Pathogenesis of type 1 and type 2 diabetes in sub-Saharan Africa: implications of transitional populations. J Cardovasc Risk 2003;10:85-96. PMID: 12668905] leading to many diseases, the nutritional transition of the immigrants is one of the causes supporting the increase of obesity, atherosclerosis, and diabetes [1010Osei K. Metabolic consequences of the West African diaspora: lessons from the thrifty-gene. J Lab Clin Mede. 1999;133:98-111. PMID: 9989761]. This situation is perhaps the exaggerated translation of the thrifty genotype [3131Rotimi CN, Dunston GM, Berg K, Akinsete O, Amoah A, Owusu S, et al. In search of susceptibility gene of type 2 diabetes in West Africa: the design and results of the first phase of the AADM study. Ann Epidemiol. 2001;11:51-58. PMID: 11164120]. The faster increase in the waist measurement than in the BMI among Nigerian immigrants [1111Okosun IS, Cooper RS, Rotimi CN, Osotimehin B, Forrester T. Association of waist circumference with risk of hypertension and type-2 diabetes in Nigerians, Jamaicans, and African-Americans. Diabetes Care. 1998;11:1836-1842. PMID: 9802730] would be another translation of this accelerated nutritional transition. However, some migrants (Tunisians) avoid this bad evolution because of their low alcohol consumption [3434Mejean C, Traissac P, Eymard-Duvernay S, El Ati J, Delpeuch F, Maire B. Influence of socio-economic and lifestyle factors on overweight and nutrition-related diseases among Tunisian migrants versus non-migrant Tunisians and French. BMC Public Health 2007; 7:265. PMCID: PMC2110891].
Another explanation is possible: the existence of a form of diabetes, border between DT-1 and DT-2, more common in Blacks and specifically in sub-Saharan Africa [3535Katte JC, Squires S, Dehayem MY, Balungi PA, Padoa CJ, Sengupta D, et al. Non-autoimmune, insulin-deficient diabetes in children and young adults in Africa: evidence from the Young-Onset Diabetes in sub-Saharan Africa (YODA) cross-sectional study. Lancet Diabetes Endocrinol. 2025;13:745-753. PMID: 40706606]. Then this evolution toward higher diabetic risk could be moderated by the interbreeding of the cultures among migrants, but would tend to be worsened by the tendency to “inter-culturality” [3636Thieblemont-Dollet S. Actes du Colloque “Lorraine, Terre d’accueil et de brassage des populations”. 2001;7:228-243.], a tendency of migrants to be less vigilant about their own nutritional habits.
Medium-term nutritional consequences in the immigration countries, as in the big cities of the Developing Countries (where the villagers leaving the camps are concentrated), are likely to have a quick and destructive effect. This raises the question of prevention with respect to the consequences of the economic transition, which could accelerate the “obesogenic transformation of the society” [3737Pedersen MM, Ekstrom CT, Sorensen TI. Emergence of the obesity epidemic preceding the presumed obesogenic transformation of society. Sci Adv. 2023;9:eadge6237. PMID: 37703366].
Study limitations
This study has several limitations. First, fasting status could not be objectively verified in all participants, particularly in rural villages, which may have affected glucose measurements. Second, venous plasma glucose and oral glucose tolerance testing were unavailable in the rural setting, requiring reliance on capillary glucose measurements. Third, the sample size of the migrant population was relatively small compared with the rural cohort. Finally, dietary intake and physical activity were not quantitatively assessed, limiting the ability to precisely evaluate lifestyle-related contributors to diabetes risk.
Senegalese migrants living in France exhibit substantially higher rates of impaired fasting glucose and diabetes compared with their relatives residing in rural Senegal. These findings strongly suggest that migration-associated environmental and lifestyle changes contribute to metabolic deterioration and increased diabetes risk. Preventive public health interventions targeting nutrition, obesity, and sedentary lifestyles among migrant populations are urgently needed.
Mbanya JCN, Sobngwi E, Assah FK, Enoru ST. Diabetes in sub-Saharan Africa. Lancet. 2010;375:2254-66. PMID: 20609971
Diabetes atlas (4th edn). International Diabetes Federation, 2006.
Sobngwi E, Mauvais-Jarvis F, Vexiau P, Mbanya JCN, Gautier JF. Diabetes in Africans, part 2: ketosis-prone atypical diabetes mellitus. Diabetes Metab. 2002;28:5-12.
Sarr A, Lopez-Sall P, Ndour-Mbaye NM, Diop SN, Sarr GN, Diop O, et al. Frequency of metabolic syndrome in Black Africans, in Senegal. Médecine des Maladies Métaboliques. 2012;6-3:238-43.
Motala AA. Diabetes trends in Africa. Diabetes Metab Res Rev. 2002;18:S14-S20. PMID: 12324980
Fontbonne A, Favier F, Papoz L. Type 2 diabetes in the world: analysis of an epidemic. Journ Annu Diabetol Hotel Dieu. 2003. PMID: 12868301
Osei K, Schuster DP, Amoah AGB, Owusu SK. Diabetes in Africa. Pathogenesis of type 1 and type 2 diabetes in sub-Saharan Africa: implications of transitional populations. J Cardovasc Risk 2003;10:85-96. PMID: 12668905
Fontbonne A, Cournil A, Cames C, Mercier S, N’Diaye-Coly A, Lacroux A, et al. Anthropometric characteristics and cardiometabolic risk factors in a sample of urban-dwelling adults in Senegal. Diabetes Metab. 2011;37:52-58. PMID: 21112227
Osei K, Schuster DE. Metabolic characteristics of African descendants: a comparative study of African-Americans and Ghanaians immigrants using minimal analysis. Diabetologia. 1995;38:1103-1109. PMID: 8591826
Osei K. Metabolic consequences of the West African diaspora: lessons from the thrifty-gene. J Lab Clin Mede. 1999;133:98-111. PMID: 9989761
Okosun IS, Cooper RS, Rotimi CN, Osotimehin B, Forrester T. Association of waist circumference with risk of hypertension and type-2 diabetes in Nigerians, Jamaicans, and African-Americans. Diabetes Care. 1998;11:1836-1842. PMID: 9802730
Haffner SM, Howard G, Mayer E, Bergmann NR, Savage PJ, Rewers M, et al. Insulin sensitivity and acute insulin response in African-Americans, non-Hispanic whites, and Hispanics with NIDDM. The insulin resistance atherosclerosis study. Diabetes. 1997;46:63-69. PMID: 8971083
Sicree RA, Zimmet PZ, Cameron AJ, Magliano DJ, Shaw JE. Diabetes prevalence among migrant populations in Australia: prevalence and risk factor associations. Diabetologia. 2008;51:S427.
Fujimoto WY. The growing prevalence of non-insulin-dependent diabetes in migrant Asian populations and its implications for Asia. Diabetes Res Clin Pract. 1992;15:167-183. PMID: 1563334
Delcourt C, Papoz L. Diabetes and its complications in the French population. Editions Inserm. 1996.
Mbanya JC, Cruickshank JF, Forrester T, Balkau B, Ngogang NY, Riste L, et al. Standardized comparison of glucose tolerance in West-African origin populations of rural and urban Cameroon, Jamaica, and Caribbean migrants to Britain. Diabetes Care. 1999;22:434-440. PMID: 10097925
Henson JJ, Gray LJ, Khunti K, Guru A, Misra A, Davies MJ. The impact of migration on metabolic outcomes and coronary heart disease risk: a comparison of migrant South Asians, Asian Indians and white Europeans. Diabetologia 2010;53:S354.
Ducorps M, Baleynaud S, Mayaudon H, Castagne C, Bauduceau B. A prevalence survey of diabetes in Mauritania. Diabetes Care. 1996;19:761-763. PMID: 8799635
Basdevant A, Laville M, Ziegler O. Practice guideline for the diagnosis, prevention, treatment of obesity in France. Diabetes Metab. 1998;24:10-42. PMID: 9805639
Summer AE, Kushner H, Tulenko TN, Falkner B, Marsch JB. The relationship in African-Americans of sex differences in insulin-mediated suppression of nonesterified fatty acids to sex differences in fasting triglyceride levels. Metabolism. 1997;46:400-405. PMID: 9109843
McLarty DG, Unwin N, Kitange HM, Alberti K. Diabetes mellitus as a cause of death in sub-Saharan Africa: results of a community-based study in Tanzania. The Adult Morbidity and Mortality Project. Diab Med. 1996;13:990-994. PMID: 8946159
Motala Ayesha A, Omar Mohammed AK, Pirie FJ. Diabetes in Africa. Epidemiology of type 1 and type 2 diabetes in Africa. J Cardiovasc Risk. 2003;10:77-83. PMID: 12668904
Brancati FL, Kao WHL, Folsom AR, Watson AR. Incident type 2 diabetes mellitus in African American and white adults: the Atherosclerosis Risk in Communities Study. JAMA. 2000;283:2253-2259. PMID: 10807384
Taylor R, Bennet P, Uili R, Joffres M, Germain R, Levy S, et al. Diabetes in Wallis Polynesian: a comparison of residents of Wallis Islands and first-generation migrants in Noumea, New Caledonia. Diab Res Clin Pract. 1985;1:169-178. PMID: 3836104
Ramachandran A, Snehalatha C, Dharmaraj D, Viswanathan M. Prevalence of glucose intolerance in Asian Indians: urban-rural differences and significance of upper body adiposity. Diabetes Care. 1992;15:1348-1355. PMID: 1425100
Papoz L, Ben Khalifa F, Eschwege E, Ayed HB. Diabetes mellitus in Tunisia: description in urban and rural populations. Int J Epidemiol. 1988;17:419-422. PMID: 3403139
Costagliola D, Delaunay C, Moutet JP, Kankambega P, Demeulemeester R, Donnet JP, et al. The prevalence of diabetes mellitus in the adult population of Guadeloupe as estimated by history or fasting hyperglycemia. Diab Res Clin Pract. 1991;12:209-16.
Connoly V, Unwin N, Sherriff P, Bilous R, Kelly W. Diabetes prevalence and socioeconomic status: a population-based study showing increased prevalence of type 2 diabetes mellitus in deprived areas. J Epid Comm Health. 2000;54:173-177. PMID: 10746110
Gautier JF, Sobngwi E, Vexiau P. How I treat and manage diabetes in black people. 19e Journées de Diabétologie de l’Hôtel-Dieu. 2001.
Buthelezi EP, Van Der Merwe MT, Lönnroth PN, Gray PI, Crowther NJ. Ethnic differences in the responsiveness of adipocyte lipolytic activity to insulin. Obes Res. 2000;8:171-178. PMID: 10757203
Rotimi CN, Dunston GM, Berg K, Akinsete O, Amoah A, Owusu S, et al. In search of susceptibility gene of type 2 diabetes in West Africa: the design and results of the first phase of the AADM study. Ann Epidemiol. 2001;11:51-58. PMID: 11164120
Ricordeau P, Weill A, Vallier N, Fender P, Allemand H. Epidemiology of diabetes in metropolitan France. Diab Metab. 2001;26:11-24. PMID: 11011236
Swinburn BA. The thrifty genotype hypothesis: how does it look after 30 years? Diab Med. 1996;13:695-699. PMID: 8862942
Mejean C, Traissac P, Eymard-Duvernay S, El Ati J, Delpeuch F, Maire B. Influence of socio-economic and lifestyle factors on overweight and nutrition-related diseases among Tunisian migrants versus non-migrant Tunisians and French. BMC Public Health 2007; 7:265. PMCID: PMC2110891
Katte JC, Squires S, Dehayem MY, Balungi PA, Padoa CJ, Sengupta D, et al. Non-autoimmune, insulin-deficient diabetes in children and young adults in Africa: evidence from the Young-Onset Diabetes in sub-Saharan Africa (YODA) cross-sectional study. Lancet Diabetes Endocrinol. 2025;13:745-753. PMID: 40706606
Thieblemont-Dollet S. Actes du Colloque “Lorraine, Terre d’accueil et de brassage des populations”. 2001;7:228-243.
Pedersen MM, Ekstrom CT, Sorensen TI. Emergence of the obesity epidemic preceding the presumed obesogenic transformation of society. Sci Adv. 2023;9:eadge6237. PMID: 37703366
Dollet JM, Soyeux L, Niang-Diene A, Guillemin F, Diop SN. Comparative Study of Glucose Abnormalities Among Senegalese Migrants and Rural Populations. IgMin Res. May 28, 2026; 4(5): 169-174. IgMin ID: igmin342; DOI:10.61927/igmin342; Available at: igmin.link/p342
1CH St-Charles, Service de Médecine A, 88100 Saint-Die, France
2Université Cheikh Anta Diop, Département de Géographie, Dakar, Sénégal
3Université de Lorraine, École de Santé Publique, 54000 Nancy, France
4Université Cheikh Anta Diop, Faculté de Médecine et Pharmacie, Dakar, Sénégal
Address Correspondence: Jean Marc Dollet, Department of Medicine A Saint-Charles Hospital Center Saint-Dié-des-Vosges, France. Email: jean-marc-dollet@wanadoo.fr
How to cite this article: Dollet JM, Soyeux L, Niang-Diene A, Guillemin F, Diop SN. Comparative Study of Glucose Abnormalities Among Senegalese Migrants and Rural Populations. IgMin Res. May 28, 2026; 4(5): 169-174. IgMin ID: igmin342; DOI:10.61927/igmin342; Available at: igmin.link/p342
Copyright: 2026 Dollet JM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Figure 1: Correlation between BMI and age (years) in Fuuta (...
Figure 2: Correlation between WHR and age (years) in Fuuta (...
Table 1: Baseline characteristics of the 2 studied populati...
Table 2: Results on glucose status for the 2 studied popula...
Mbanya JCN, Sobngwi E, Assah FK, Enoru ST. Diabetes in sub-Saharan Africa. Lancet. 2010;375:2254-66. PMID: 20609971
Diabetes atlas (4th edn). International Diabetes Federation, 2006.
Sobngwi E, Mauvais-Jarvis F, Vexiau P, Mbanya JCN, Gautier JF. Diabetes in Africans, part 2: ketosis-prone atypical diabetes mellitus. Diabetes Metab. 2002;28:5-12.
Sarr A, Lopez-Sall P, Ndour-Mbaye NM, Diop SN, Sarr GN, Diop O, et al. Frequency of metabolic syndrome in Black Africans, in Senegal. Médecine des Maladies Métaboliques. 2012;6-3:238-43.
Motala AA. Diabetes trends in Africa. Diabetes Metab Res Rev. 2002;18:S14-S20. PMID: 12324980
Fontbonne A, Favier F, Papoz L. Type 2 diabetes in the world: analysis of an epidemic. Journ Annu Diabetol Hotel Dieu. 2003. PMID: 12868301
Osei K, Schuster DP, Amoah AGB, Owusu SK. Diabetes in Africa. Pathogenesis of type 1 and type 2 diabetes in sub-Saharan Africa: implications of transitional populations. J Cardovasc Risk 2003;10:85-96. PMID: 12668905
Fontbonne A, Cournil A, Cames C, Mercier S, N’Diaye-Coly A, Lacroux A, et al. Anthropometric characteristics and cardiometabolic risk factors in a sample of urban-dwelling adults in Senegal. Diabetes Metab. 2011;37:52-58. PMID: 21112227
Osei K, Schuster DE. Metabolic characteristics of African descendants: a comparative study of African-Americans and Ghanaians immigrants using minimal analysis. Diabetologia. 1995;38:1103-1109. PMID: 8591826
Osei K. Metabolic consequences of the West African diaspora: lessons from the thrifty-gene. J Lab Clin Mede. 1999;133:98-111. PMID: 9989761
Okosun IS, Cooper RS, Rotimi CN, Osotimehin B, Forrester T. Association of waist circumference with risk of hypertension and type-2 diabetes in Nigerians, Jamaicans, and African-Americans. Diabetes Care. 1998;11:1836-1842. PMID: 9802730
Haffner SM, Howard G, Mayer E, Bergmann NR, Savage PJ, Rewers M, et al. Insulin sensitivity and acute insulin response in African-Americans, non-Hispanic whites, and Hispanics with NIDDM. The insulin resistance atherosclerosis study. Diabetes. 1997;46:63-69. PMID: 8971083
Sicree RA, Zimmet PZ, Cameron AJ, Magliano DJ, Shaw JE. Diabetes prevalence among migrant populations in Australia: prevalence and risk factor associations. Diabetologia. 2008;51:S427.
Fujimoto WY. The growing prevalence of non-insulin-dependent diabetes in migrant Asian populations and its implications for Asia. Diabetes Res Clin Pract. 1992;15:167-183. PMID: 1563334
Delcourt C, Papoz L. Diabetes and its complications in the French population. Editions Inserm. 1996.
Mbanya JC, Cruickshank JF, Forrester T, Balkau B, Ngogang NY, Riste L, et al. Standardized comparison of glucose tolerance in West-African origin populations of rural and urban Cameroon, Jamaica, and Caribbean migrants to Britain. Diabetes Care. 1999;22:434-440. PMID: 10097925
Henson JJ, Gray LJ, Khunti K, Guru A, Misra A, Davies MJ. The impact of migration on metabolic outcomes and coronary heart disease risk: a comparison of migrant South Asians, Asian Indians and white Europeans. Diabetologia 2010;53:S354.
Ducorps M, Baleynaud S, Mayaudon H, Castagne C, Bauduceau B. A prevalence survey of diabetes in Mauritania. Diabetes Care. 1996;19:761-763. PMID: 8799635
Basdevant A, Laville M, Ziegler O. Practice guideline for the diagnosis, prevention, treatment of obesity in France. Diabetes Metab. 1998;24:10-42. PMID: 9805639
Summer AE, Kushner H, Tulenko TN, Falkner B, Marsch JB. The relationship in African-Americans of sex differences in insulin-mediated suppression of nonesterified fatty acids to sex differences in fasting triglyceride levels. Metabolism. 1997;46:400-405. PMID: 9109843
McLarty DG, Unwin N, Kitange HM, Alberti K. Diabetes mellitus as a cause of death in sub-Saharan Africa: results of a community-based study in Tanzania. The Adult Morbidity and Mortality Project. Diab Med. 1996;13:990-994. PMID: 8946159
Motala Ayesha A, Omar Mohammed AK, Pirie FJ. Diabetes in Africa. Epidemiology of type 1 and type 2 diabetes in Africa. J Cardiovasc Risk. 2003;10:77-83. PMID: 12668904
Brancati FL, Kao WHL, Folsom AR, Watson AR. Incident type 2 diabetes mellitus in African American and white adults: the Atherosclerosis Risk in Communities Study. JAMA. 2000;283:2253-2259. PMID: 10807384
Taylor R, Bennet P, Uili R, Joffres M, Germain R, Levy S, et al. Diabetes in Wallis Polynesian: a comparison of residents of Wallis Islands and first-generation migrants in Noumea, New Caledonia. Diab Res Clin Pract. 1985;1:169-178. PMID: 3836104
Ramachandran A, Snehalatha C, Dharmaraj D, Viswanathan M. Prevalence of glucose intolerance in Asian Indians: urban-rural differences and significance of upper body adiposity. Diabetes Care. 1992;15:1348-1355. PMID: 1425100
Papoz L, Ben Khalifa F, Eschwege E, Ayed HB. Diabetes mellitus in Tunisia: description in urban and rural populations. Int J Epidemiol. 1988;17:419-422. PMID: 3403139
Costagliola D, Delaunay C, Moutet JP, Kankambega P, Demeulemeester R, Donnet JP, et al. The prevalence of diabetes mellitus in the adult population of Guadeloupe as estimated by history or fasting hyperglycemia. Diab Res Clin Pract. 1991;12:209-16.
Connoly V, Unwin N, Sherriff P, Bilous R, Kelly W. Diabetes prevalence and socioeconomic status: a population-based study showing increased prevalence of type 2 diabetes mellitus in deprived areas. J Epid Comm Health. 2000;54:173-177. PMID: 10746110
Gautier JF, Sobngwi E, Vexiau P. How I treat and manage diabetes in black people. 19e Journées de Diabétologie de l’Hôtel-Dieu. 2001.
Buthelezi EP, Van Der Merwe MT, Lönnroth PN, Gray PI, Crowther NJ. Ethnic differences in the responsiveness of adipocyte lipolytic activity to insulin. Obes Res. 2000;8:171-178. PMID: 10757203
Rotimi CN, Dunston GM, Berg K, Akinsete O, Amoah A, Owusu S, et al. In search of susceptibility gene of type 2 diabetes in West Africa: the design and results of the first phase of the AADM study. Ann Epidemiol. 2001;11:51-58. PMID: 11164120
Ricordeau P, Weill A, Vallier N, Fender P, Allemand H. Epidemiology of diabetes in metropolitan France. Diab Metab. 2001;26:11-24. PMID: 11011236
Swinburn BA. The thrifty genotype hypothesis: how does it look after 30 years? Diab Med. 1996;13:695-699. PMID: 8862942
Mejean C, Traissac P, Eymard-Duvernay S, El Ati J, Delpeuch F, Maire B. Influence of socio-economic and lifestyle factors on overweight and nutrition-related diseases among Tunisian migrants versus non-migrant Tunisians and French. BMC Public Health 2007; 7:265. PMCID: PMC2110891
Katte JC, Squires S, Dehayem MY, Balungi PA, Padoa CJ, Sengupta D, et al. Non-autoimmune, insulin-deficient diabetes in children and young adults in Africa: evidence from the Young-Onset Diabetes in sub-Saharan Africa (YODA) cross-sectional study. Lancet Diabetes Endocrinol. 2025;13:745-753. PMID: 40706606
Thieblemont-Dollet S. Actes du Colloque “Lorraine, Terre d’accueil et de brassage des populations”. 2001;7:228-243.
Pedersen MM, Ekstrom CT, Sorensen TI. Emergence of the obesity epidemic preceding the presumed obesogenic transformation of society. Sci Adv. 2023;9:eadge6237. PMID: 37703366



 Scan and get link
Scan and get link